Horse colic surgery is one of the most urgent decisions you may ever face as a horse owner, and recognizing when your horse truly needs it can mean the difference between recovery and tragedy. Colic remains the leading medical cause of death in horses worldwide, yet the majority of surgical cases are highly survivable when caught early enough.
This guide gives you the practical knowledge to spot a true surgical emergency, understand how your veterinarian reaches the decision, and walk your horse through every stage of recovery with confidence.
You will learn the five red flag signs that drive most referrals, the common lesions surgeons encounter on the operating table, and the prognosis numbers backed by current peer reviewed research. The information here reflects the standards taught at leading veterinary teaching hospitals and published by the American Association of Equine Practitioners.
Time is the most precious resource in any colic case. Research in the Equine Veterinary Journal shows survival rates above eighty five percent when horses reach the operating room within four hours of symptom onset. Delays beyond twelve hours can cut those numbers nearly in half.
Picture this: a calm Tuesday evening turns into a midnight ride to the equine hospital. The decisions you make in those first sixty minutes shape everything that follows. Knowing exactly what to watch for transforms panic into purposeful action.
What follows is a comprehensive walkthrough designed for horse owners. You will learn how surgeons think and what your role looks like from first pawing to full return to work.
Key Takeaways
- Severe pain unresponsive to banamine signals likely surgical colic
- Heart rates above sixty beats per minute indicate developing shock
- Strangulating lesions require surgical correction within hours of onset
- Modern survival rates exceed eighty percent with timely referral
- Most horses return to full work within six months of surgery
Understanding Colic: Medical vs Surgical Emergencies
Colic refers to any abdominal pain in horses, but the term covers a vast spectrum of conditions. Some episodes resolve with a single dose of pain medication, while others demand the operating table within ninety minutes.
The American Association of Equine Practitioners estimates that roughly ninety percent of colic cases respond fully to medical care alone. The remaining ten percent fall into surgical territory, where mechanical or vascular emergencies require direct surgical intervention.
Understanding which category your horse falls into starts with knowing what is happening inside the abdomen and why the equine gut is uniquely vulnerable to crisis.
What is Equine Colic and Why Does It Escalate?
Equine colic is an umbrella term for gastrointestinal pain originating anywhere from the stomach to the rectum. Because horses cannot vomit and have a long, mobile small intestine suspended by a delicate mesentery, even modest disruptions can cascade quickly into a true equine gastrointestinal emergency.
The horse’s digestive system depends on constant motility. When that motion slows or a segment becomes trapped, gas accumulates, pressure builds, and blood supply weakens. Within hours, intestinal tissue can begin to die.
Here is the key thing to remember: horses do not tolerate intestinal stillness for long. The Merck Veterinary Manual notes that strangulating obstructions develop irreversible tissue death in as little as three to six hours, which is why early recognition is non negotiable.
Common triggers include sudden feed changes, sand ingestion, internal parasites, dehydration, dental problems, and stress related ulcers. Even temperature swings, transport stress, or pasture turnout after stall confinement can disrupt gut motility enough to set off an episode.
Mild Discomfort vs Life Threatening Intestinal Issues
Most colic episodes start with mild signs of colic in horses: pawing, sweating, lying down, repeatedly looking at the flank, or stretching as if to urinate. About ninety percent of these episodes resolve with banamine, fluids, and time. The clinical challenge is identifying the ten percent that will not.
Think of it this way: two horses arrive at the clinic with identical dull pain. One has gas distension in the cecum that will pass in two hours. The other has a small intestinal volvulus that will be fatal within six hours. They look similar in the first sixty minutes, but their outcomes diverge dramatically.
Surgical colic in horses is any abdominal emergency where the intestinal tract becomes mechanically obstructed, strangulated, or displaced beyond the reach of medical therapy, requiring an immediate exploratory laparotomy to save the horse’s life and restore normal gut function.
The Texas A&M College of Veterinary Medicine teaches its students to track three changes over time: pain severity, vital sign trends, and gut motility. If all three move in the wrong direction, surgery shifts from possible to probable. The bottom line is this: surgical colic is defined by progression, not by a single static symptom.
Worth noting is that mild cases can transform into surgical emergencies within hours. A simple gas colic at breakfast can become a displaced colon by lunchtime. Continuous monitoring across the first twelve hours is essential.
Your veterinarian uses a layered approach to separate these two worlds. The first layer is the physical exam, the second is pain response to medication, and the third is the laboratory and ultrasound workup. When all three layers point in the same direction, the diagnostic path becomes clear and the next move becomes obvious.
5 Critical Signs Your Horse Needs Immediate Colic Surgery
The fastest path to recognizing surgical colic is memorizing the red flag cluster. Vets do not rely on a single symptom; they look for combinations that signal mechanical or vascular compromise. The five signs below drive the majority of surgical referrals across North America and Europe.
Make no mistake: if you observe two or more of these signs at once, call your veterinarian immediately and prepare for transport. Hesitation kills horses.
Uncontrollable Pain That Responds Poorly to Banamine
Banamine, the brand name for flunixin meglumine, is the standard analgesic for equine colic. When a normal field dose fails to relieve pain within thirty minutes, the cause is rarely a simple medical issue.
A horse that returns to thrashing, pawing, or violent rolling soon after injection is telling you the lesion is mechanical, not spasmodic. Most surgical referrals begin with this single observation. The bottom line is this: refractory pain almost always means a strangulating or obstructive lesion that medication cannot relieve.
Banamine for horses works by blocking inflammation and pain transmission. It does not fix twisted bowel, displaced colons, or strangulating lipomas. When the drug fails, the lesion is structural, not chemical.
Some veterinarians use a second test dose of detomidine or xylazine before declaring pain refractory. If even strong sedatives fail to settle a horse for more than fifteen minutes, the surgical case is essentially confirmed.
High Heart Rate and Pale Gums (Signs of Shock)
A resting heart rate above sixty beats per minute, combined with pale or muddy gum color and a capillary refill time over two seconds, signals circulatory shock. These are textbook horse shock symptoms.
Shock develops when toxins from compromised intestine leak into the bloodstream. The horse’s body shunts blood away from peripheral tissues, including the mucous membranes of the gums. This is your animal’s internal emergency dashboard light, and ignoring it is often fatal.
Veterinarians at the New Bolton Center at the University of Pennsylvania consider a sustained heart rate of eighty or more a strong predictor of strangulation. Pair that with prolonged capillary refill and the surgical likelihood rises sharply.
Track horse heart rate during colic every fifteen minutes. A rising trend, even within the normal range, is more informative than a single number in isolation. Write each reading down with the time, since memory fades quickly during a stressful event.
Capillary refill time is easy to check yourself. Press your thumb firmly against the upper gum for two seconds, then release. Color should return within one to two seconds. Anything slower indicates poor perfusion.
Large Volume of Gastric Reflux via Stomach Tube
When your vet passes a nasogastric tube and recovers more than two liters of fluid, an obstruction in the small intestine is highly likely. The reflux is a backup of digestive juice that cannot pass downstream because of a blockage or paralysis.
Persistent gastric reflux in horses of four liters or more virtually confirms a small intestinal strangulation or proximal enteritis, both of which often require surgery. Reflux also relieves dangerous pressure, so the procedure doubles as a diagnostic and a temporary lifesaver.
But here is where most horse owners go wrong: they assume a horse that stops rolling has improved. In reality, a sudden quiet phase can mean the bowel has stopped sending pain signals because the tissue is dying. Reflux production tells the real story.
Once reflux is established, your vet may leave the nasogastric tube in place for transport, taped to the halter, so fluid can drain continuously. This single intervention often makes the difference between a horse that survives the trailer ride and one that does not.
Silent Gut Sounds: What an Absence of Noise Means
Healthy horses produce continuous gurgling sounds across all four abdominal quadrants. When your vet listens with a stethoscope and hears total silence, the gut has stopped moving.
Think of it this way: a quiet gut is a paralyzed gut. Mechanical obstruction, severe distension, and shock all shut down peristalsis. The longer the silence, the higher the surgical likelihood.
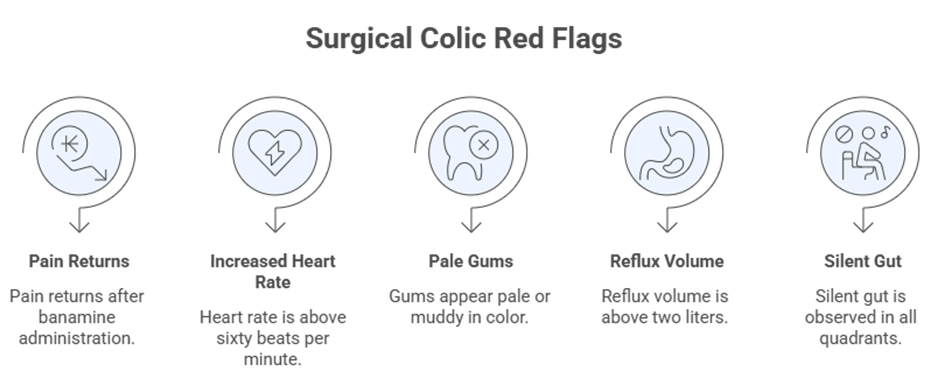
Use this numbered checklist when you assess your horse before the vet arrives. If three or more items apply, treat the case as a true emergency colic in horses and prepare the trailer.
- Pain returns within thirty minutes of banamine injection
- Heart rate climbs above sixty beats per minute
- Mucous membranes turn pale, muddy, or purple
- Gastric reflux exceeds two liters on nasogastric tubing
- Gut sounds disappear in all four abdominal quadrants
- Sweating, trembling, or repeated violent rolling continues
- Abdominal distension visibly worsens within two hours
Common Types of Surgical Colic in Horses
Not every surgical colic looks the same on the operating table. Surgeons encounter a handful of recurring lesions, each with its own warning pattern, age profile, and prognosis. Understanding these patterns helps you communicate clearly with your veterinarian and make informed decisions.
The three categories below account for the majority of surgical referrals. Knowing them does not change the immediate response, but it sharpens your conversations during diagnosis and recovery.
Twisted Gut (Volvulus and Torsion)
Volvulus describes a complete rotation of a segment of intestine on its own axis. Large colon volvulus is the most dramatic version, often turning one hundred eighty or three hundred sixty degrees. Intestinal torsion in horses is among the most painful and time sensitive surgical emergencies in veterinary medicine.
When the colon flips, blood vessels in the mesentery pinch shut. Tissue death begins almost immediately, and the horse experiences violent, uncontrollable pain. Surgery is the only path forward, and timing decides everything.
But here is where most horse owners go wrong: they assume a horse that briefly settles after rolling has improved. In reality, a sudden quiet phase often means the bowel has lost feeling because it is dying. The window for successful correction may be closing, not opening.
Mares in late pregnancy or the first ninety days postpartum carry the highest risk of large colon volvulus. The Royal Veterinary College in London reports survival rates of seventy to eighty percent when these cases reach surgery within two hours.
Small intestinal volvulus is less common but equally dangerous. It often occurs in young foals during periods of rapid intestinal growth, or in adult horses after sudden dietary shifts. The clinical signs match the most severe profile imaginable: violent pain, profound shock, and rapid deterioration.
Strangulating Lipomas (Fatty Tumors in Older Horses)
Pedunculated strangulating lipoma growths are benign fatty masses attached to the mesentery by a long stalk. In horses over fifteen years old, these stalks can wrap around the small intestine like a noose, cutting off blood supply within hours.
Once strangulation begins, the affected intestinal segment loses blood supply rapidly. Studies from the Royal Veterinary College show lipomas account for up to thirty percent of small intestinal surgical lesions in horses over twenty years old.
Here is the truth: older geldings of stock breeds appear most vulnerable. If your senior horse develops sudden, severe pain with no obvious trigger, suspect a strangulating lipoma until proven otherwise.
The lesion is invisible on rectal exam in most cases, which is why abdominocentesis and lactate testing become essential diagnostic tools. Time from onset to surgery is the single biggest survival factor.
Prevention is limited but real. Maintain ideal body condition in older horses, avoid sudden caloric increases, and keep your horse on a consistent forage schedule. These habits do not eliminate lipomas, but they may slow their growth.
Severe Impactions That Resist Medical Treatment
Pelvic flexure impactions are common and usually clear with intravenous fluids, mineral oil, and time. Impaction colic treatment succeeds in the majority of cases without surgery. But when an impaction sits unmoved for thirty six hours or causes worsening pain, surgery may be needed to manually evacuate the mass.
Sand impactions and ileal impactions are far tougher. The Texas A&M College of Veterinary Medicine reports that sand cases not responding to forty eight hours of medical care often progress to surgical evacuation to prevent rupture of the colon.
Consider this: impactions become surgical when they shift from a passive blockage to active tissue damage. The threshold is usually time plus pain that escalates rather than fades. A horse that stops eating and drinking entirely after twenty four hours of medical care is on the surgical pathway.
Hydration status changes the calculus too. A dehydrated horse with a stubborn impaction may need surgery sooner than a well hydrated horse with the same lesion, because dry contents become harder to break down. Many emergency hospitals begin aggressive intravenous fluid therapy immediately on arrival to rehydrate the contents and buy time.
The Vet’s Decision: How Clinicians Diagnose Surgical Cases
Veterinarians weigh several data points before recommending the operating table. The decision is rarely based on a single sign, vital trend, or test result. Instead, your vet builds a clinical picture using physical exam findings, ultrasound, blood values, and direct sampling of abdominal fluid.
The bottom line is this: surgical decisions are made by pattern recognition. Three or more red flags pointing in the same direction tip the balance toward referral.
What the Vet Looks for During a Rectal Exam
A rectal examination in horses is the cornerstone of equine colic assessment. Your vet wears a long protective sleeve, lubricates carefully, and palpates the rear quarter of the abdomen for distended loops, masses, displacements, or tight bands.
Distended small intestine feels like a tight inner tube under pressure. A displaced large colon may be palpable in an abnormal position high in the abdomen. Any of these findings raises the surgical suspicion sharply.
A rectal exam in horses is a manual abdominal palpation performed through the rectum, allowing the veterinarian to feel intestinal distension, masses, displacements, and strangulating lesions that confirm whether colic surgery is needed within the available time window.
Vets cannot reach every part of the abdomen rectally. Cranial lesions in the small intestine and parts of the colon remain hidden. That limitation is why your veterinarian often combines rectal findings with ultrasound and abdominocentesis.
Belly Tap (Abdominocentesis) and Fluid Analysis
Abdominocentesis in horses, also called a belly tap, involves inserting a small needle into the lowest point of the abdomen to collect peritoneal fluid. Normal fluid is clear and straw colored, with low protein and low cell counts.
Serosanguineous or red tinged fluid indicates blood leakage from compromised intestine. A protein concentration above twenty five grams per liter, combined with elevated lactate, often confirms a strangulating lesion. According to the Merck Veterinary Manual, lactate over six millimoles per liter strongly predicts the need for surgery.
Many clinics now run stallside lactate readings in under a minute. This rapid feedback can shave precious time off the decision window, which is critical because every hour of delay compounds the risk.
Together, rectal findings, abdominocentesis results, vital signs, pain response, and ultrasound build the diagnostic picture. If three or more red flags align, your veterinarian will recommend immediate referral to a surgical hospital.
Transcutaneous abdominal ultrasound has become the fastest growing diagnostic tool in equine colic care. With a portable probe, your vet can visualize distended small intestinal loops, free abdominal fluid, and the position of the colon within minutes. The Cornell University College of Veterinary Medicine considers ultrasound a standard part of every colic workup today.
Blood work also matters. A packed cell volume above forty five percent, combined with high total protein, signals dehydration and tissue compromise. These values become powerful prognostic indicators before and after surgery.
Colic Surgery Prognosis and Recovery Timeline
Outcomes for horse colic surgery have improved dramatically over the past three decades. Modern protocols, better imaging, faster referral systems, and refined anesthesia have lifted survival rates to levels that surprised earlier generations of equine surgeons. Colic prognosis in horses today depends largely on timing and lesion type.
The reality is that the surgery itself is no longer the biggest threat. Delay before surgery, postoperative complications, and underlying disease now drive most of the bad outcomes.
What is the Survival Rate for Equine Colic Surgery?
For large colon surgeries, short term survival rates exceed eighty five percent at most referral hospitals. Small intestinal cases vary more, ranging from sixty five to eighty percent depending on the lesion type, the length of bowel that must be resected, and time elapsed before surgery.
The Equine Veterinary Journal published a major review in 2024 showing horses referred within four hours had a survival advantage of nearly twenty five percentage points over those delayed beyond eight hours. The same review found that horses with strangulating lesions had the most to gain from early referral.
Here is the truth: most horses that reach surgery alive and stable walk out of the hospital several weeks later. The biggest predictor of failure is delay, not the operation itself. Survival rate of colic surgery climbs sharply when owners act decisively.
Insurance status also influences outcomes indirectly. Owners with mortality and major medical coverage make faster decisions because the financial barrier is removed. This is one practical reason equine insurance is worth careful consideration before a crisis ever arrives.
Geographic proximity to a referral hospital is another silent variable. Horses living within a sixty minute drive of a surgical center have measurably better outcomes than those requiring three or four hours of trailering. If you live in a remote area, ask your veterinarian to map out the closest options now, before any emergency develops.
Postoperative Care: Stall Rest and Reintroducing Feed
Recovery from horse abdominal surgery happens in carefully staged phases. The first seventy two hours are the most critical, while the full return to athletic work spans roughly six months. Postoperative horse care is a partnership between your veterinarian, hospital staff, and you.
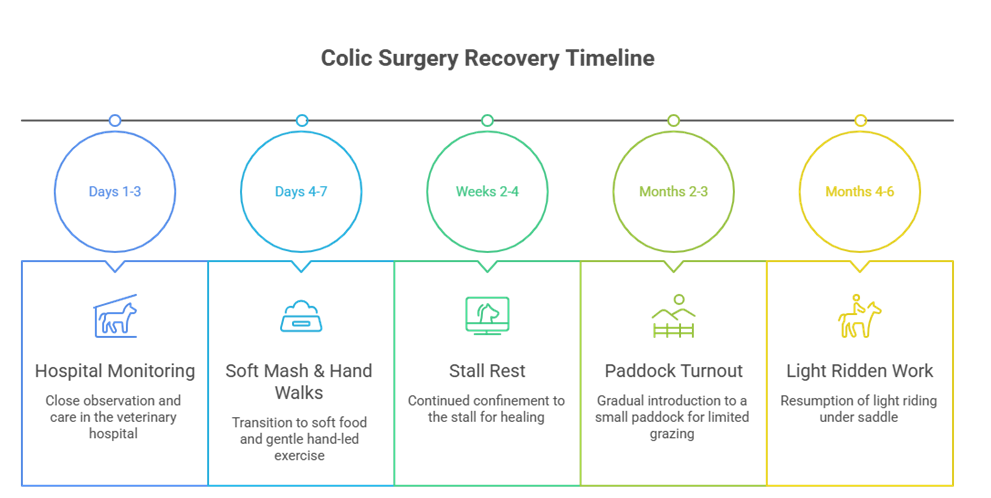
Standard colic surgery recovery timeline by stage:
- Days 1 to 3: Hospital monitoring, intravenous fluids, gradual water reintroduction
- Days 4 to 7: Soft mash diet, gentle hand walking inside the stall
- Weeks 2 to 4: Continued stall rest after surgery, short hand walks twice daily
- Months 2 to 3: Small paddock turnout, gradual reintroduction of soft hay
- Months 4 to 6: Light ridden work, progressive conditioning and fitness
- Month 6 onward: Return to full athletic performance and competition
Picture this: your horse comes home with a long incision running along the midline, a clipped belly, and strict instructions for confined rest. The next ninety days will test your patience, but adherence to the plan determines whether your horse returns to full work.
Daily routines matter enormously. Check the incision twice each day for swelling, heat, or discharge. Take rectal temperature each morning and evening. Record manure piles, water intake, and appetite in a simple notebook. These small habits catch problems before they escalate, and they give your veterinarian objective data during follow up visits.
Comparison Table: Medical vs Surgical Colic at a Glance
The table below summarizes how medical vs surgical colic cases differ across the most important clinical markers. Most veterinarians use this kind of scorecard mentally when triaging horses in the field. It does not replace a hands on examination, but it helps owners understand what their vet is weighing.
| Clinical Marker | Medical Colic | Surgical Colic |
| Pain response to banamine | Resolves within thirty minutes | Returns or worsens quickly |
| Heart rate | Below sixty beats per minute | Above sixty beats per minute |
| Mucous membranes | Pink and moist | Pale, muddy, or injected |
| Gastric reflux on tube | Less than two liters | More than two liters |
| Gut sounds | Present in most quadrants | Greatly reduced or silent |
| Abdominal fluid color | Clear, low protein | Bloody, high protein and lactate |
| Typical outcome | Resolves in hours with care | Requires laparotomy within hours |
This side by side view reflects the standard approach taught at major veterinary teaching hospitals. Use it as a thinking aid when you call your vet at three in the morning, never as a substitute for professional examination.
Keep a printed copy of this comparison in your barn first aid binder. Scanning a familiar layout is easier than recalling details under stress. Your veterinarian will appreciate hearing you describe findings in clinical language, since it speeds up triage.
Horse Colic Surgery FAQs
How much does horse colic surgery typically cost in the United States?
Colic surgery in the United States generally costs between seven thousand and fifteen thousand dollars, depending on the lesion type, hospital, and complications. Costs include the procedure, general anesthesia, hospitalization for five to ten days, medications, and routine follow up care. Major referral centers in metropolitan areas may charge more, while smaller regional hospitals can be slightly less expensive. Many owners carry mortality and major medical insurance that helps offset the bill. Your veterinarian or referral hospital can usually provide a written estimate before the operation begins, which gives you a clearer picture of the financial commitment.
Can a horse return to full work and athletic performance after colic surgery?
Yes, most horses return to their previous performance level after a successful colic surgery. A study published in the Journal of the American Veterinary Medical Association reported that more than seventy percent of competitive horses resumed full work within six to nine months. Recovery depends on the lesion type, the horse’s age, body condition, and the quality of postoperative care. Sport horses, racehorses, and pleasure horses have all returned to top competitive form, though some require modified conditioning programs to rebuild strength gradually. Realistic expectations and a slow reintroduction to work yield the best long term results.
How long does a horse take to recover from colic surgery completely?
Total recovery from horse intestinal surgery typically spans six months from operation to return to full athletic work. The first two weeks involve strict stall rest and slow reintroduction of soft feed. Weeks three through six allow short hand walks and small paddock turnout under close supervision. From month three onward, light ridden work begins under veterinary guidance. By month six, most horses have returned to full athletic conditioning. Some complicated cases, such as those involving large bowel resections or postoperative complications, may need eight to twelve months for complete return to performance.
How can horse owners prevent postoperative colic complications during recovery?
Owners can sharply reduce postoperative complications by following four core habits: maintain a strict feeding schedule with frequent small meals, provide unlimited fresh clean water at all times, monitor manure output daily for the first month, and report any change in attitude or appetite to your veterinarian immediately. Avoid sudden feed changes, parasite reinfection, and pasture overload during the early recovery window. Routine deworming, regular dental care, and gentle progressive reconditioning all help prevent adhesions, ileus, and recurrence of colic episodes in the months ahead.
Is age a deciding factor when choosing colic surgery for an older horse?
Age alone is not a disqualifier for colic surgery. Horses in their twenties have successfully recovered from major procedures, particularly when general health is good and the underlying lesion is correctable. The deciding factors are body condition, comorbidities such as Cushing’s disease or laminitis, and the specific lesion involved. The Royal Veterinary College has reported survival rates above seventy percent in geriatric horses given timely surgery. Your veterinarian weighs quality of life, recovery capacity, and prognosis together when advising older owners. Many senior horses live productive lives for years after surgery.
What are the warning signs of colic surgery complications during recovery?
Watch for fever above one hundred two degrees Fahrenheit, swelling or discharge at the incision site, sudden loss of appetite, decreased manure output, lethargy, or recurrence of abdominal pain. Adhesions, ileus, incisional hernias, and secondary laminitis are the most common postoperative complications. Daily incision checks, careful diet management, and consistent vital sign monitoring catch most issues early enough for medical intervention. Call your veterinarian at the first sign of any deviation from normal recovery patterns. Early reporting is the single best protection against minor issues becoming major emergencies.
Can colic surgery be safely repeated if a horse colics again?
Yes, horses can undergo colic surgery more than once, although repeat operations carry slightly higher risks due to adhesions and scar tissue from the first procedure. The decision depends on the underlying cause of the second episode, the horse’s general health, and the time interval between operations. Many horses recover well from second surgeries when the cause is corrected and postoperative protocols are followed carefully. Always discuss prevention strategies, parasite control, and feeding management with your veterinarian to reduce the risk of future episodes and improve long term gut health.
Horse colic surgery is one of the most demanding emergencies in equine medicine, but recognizing the right signs and acting fast can save your horse’s life. Severe pain unresponsive to banamine, a rising heart rate, gastric reflux, silent gut sounds, and signs of shock together demand immediate veterinary referral. No single sign is decisive on its own, but a cluster of three or more should send you straight to the trailer with the engine running.
The science is clear on one point: time is the variable you control. Survival rates exceed eighty percent with early surgical intervention, and the vast majority of horses go on to return to their work, sport, or pleasure roles. Your role as an owner is to know the warning signs, trust your instincts, monitor your horse closely, and call your veterinarian without hesitation when something feels wrong.
Every horse and every colic case is unique, and the decision to operate involves dozens of variables only your veterinarian can fully assess in person. The information here will help you ask better questions and respond more confidently, but it does not replace a hands on examination by a licensed professional who knows your horse. Please consult your veterinarian or a certified equine surgeon for advice tailored to your horse’s individual needs, medical history, and current condition.